

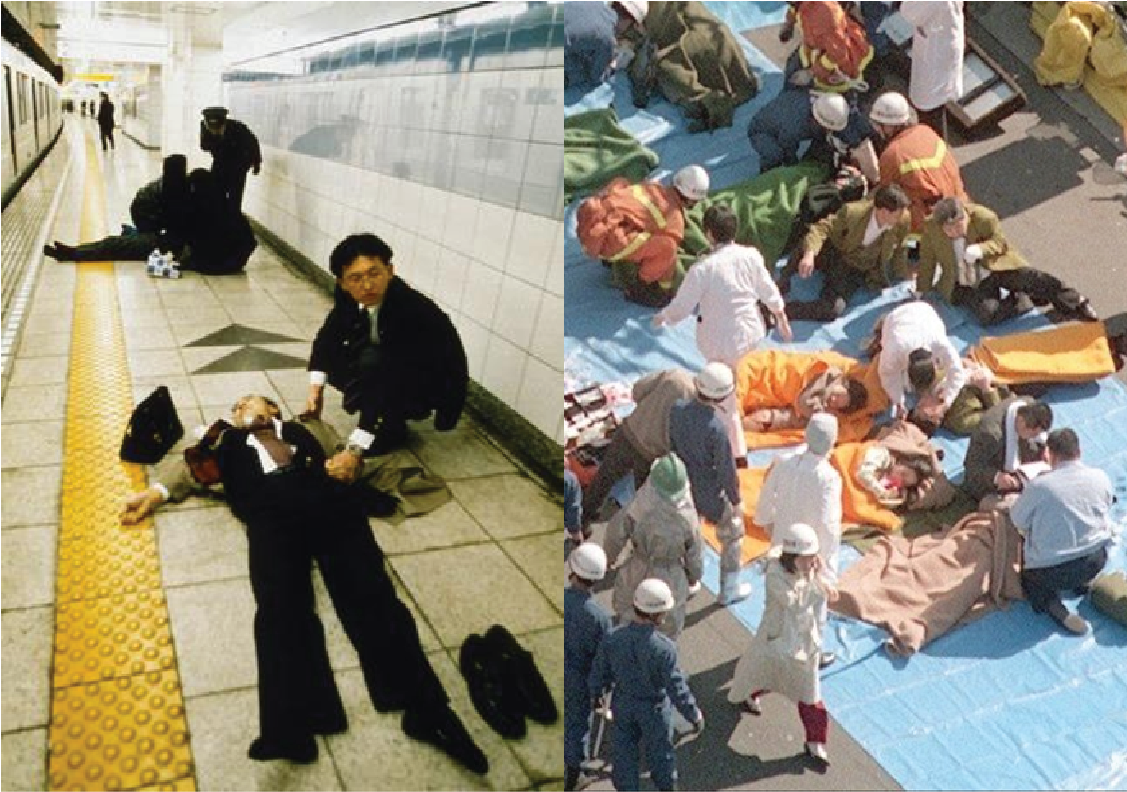
The aftermath of Aum Shinrikyo’s 1995 attack in the Tokyo subway with the chemical warfare agent sarin demonstrated the consequences of inadequate communication with the public and response partners during a large-scale chemical incident. First, civilians, transit authorities, and first-responders that individually became aware of a critical problem were slow to report it or to coordinate action. For example, although the subway train control center was notified of a critical issue, trains were allowed to continue on their scheduled routes, resulting in the contamination of multiple train lines, fifteen stations, and hundreds of people. In fact, it was roughly forty minutes into the response before orders went out from the police requiring that rescuers entering the subway system wear gas masks.
Essential components of the medical system were crippled by inadequate communications systems. As the event escalated, the sheer number of rescue vehicles activated clogged regular communications channels. Ambulance crews were unable to get through to the dispatch center to determine which hospitals could receive patients; some even stopped at pay telephones to try to secure instructions directly from hospitals.
Further, essential incident information was not delivered to Tokyo hospitals. Doctors at one hospital located near the affected subway stations reported receiving no information from city fire or police departments about what was occurring—they heard only that there might have been an explosion in the subway system—and were forced to rely upon television news reports for event details. Due to the information vacuum, the decision to expand emergency medical operations to include the entire staff was delayed, and it was roughly two and a half hours after the first affected person reached their doorstep that the hospital’s staff finally learned—again from television broadcasts, not through official channels—that the toxic substance involved was sarin. Only then did hospital staff began to administer the appropriate nerve agent antidote treatment to injured patients.
Aum Shinrikyo’s attack also made clear how communications between experts and responding partners can be critical for the dissemination of potentially lifesaving information during a chemical incident. In particular, a physician familiar with treating patients exposed to sarin called hospitals during the attack in Tokyo to alert them that the symptoms he was seeing on television mirrored those he had seen during a previous attack. He also assisted medical staff near subway sites in making the diagnosis of sarin exposure. Given the lack of information flow to hospitals, his expertise was likely lifesaving. From the attack, Tokyo officials and physicians learned the importance of pre-planning and the need to pre-identify and link the range of experts that responses to certain situations might demand.
In Tokyo, crisis response communications of civil and government organizations were not effectively coordinated, and in some cases experienced technological failures. In addition, the absence of immediate and clear information delivery to the public led to medical facilities being overwhelmed with patients who were at little to no risk of experiencing illness. Overall, public safety and services suffered.
Footnotes
22. Levy, L., Smithson, A.E. (2000). Rethinking the Lessons of Tokyo. Ataxia: The Chemical and Biological Terrorism Threat and the US Response Stimson Report 35. (pp. 71-111). Global Health Security.
32. Federal Emergency Management Agency. (2019, October 28). National Response Framework. Department of Homeland Security. 4th ed.